
1 October 2015:

3rd Year Students role-play how to educate a patient in class
Wow, I can hardly believe another month has passed as today we enter October. I think I’ve just gotten used to writing 2015 but soon it will be 2016. This also means my visit here is coming to an end. The past few days have been really busy for me and the students. On Tuesday, I taught the Pharmaceutical Care Skills Lab (PCSL) course again for the 3rd year students but Cathy taught the 4th years and did a fantastic job. I think she is ready to go on without me.

3rd Year Students role-play how to educate a patient in class
We had to hold the class in a large lecture hall this time due to another meeting in our usual room, hence the difference in the pictures.

3rd Year Students role-play how to educate a patient in class
On Wednesday, Cathy and I precepted the 4th year students during ward rounds at Mulago Hospital and then later in the day, we welcomed another American Pharmacist to Kampala.
Susan Raber and Freddy Kitutu, one of the Makerere University Faculty Members
Susan Raber has been working in Uganda on and off since 2008. She started her original work here teaching Pharmacokinetics at Makerere Pharmacy School as a Pfizer Global Health Scholar when she spent about 6 months here. Since then she has made numerous trips back to Kampala as a volunteer Pharmacist and Pharmacy Faculty member with Healthcare Volunteers Overseas (HVO). She was here last year as well and helped to teach the PCSL and precept pharmacy students and pharmacy Interns at Mulago Hospital. Susan and I have known each other by email and by phone calls for a couple of years now but this is the first time we’ve been able to meet in person. She currently works in the Clinical Pharmacology Division for Pfizer and she is an expert in Pharmacokinetics/ Pharmacodynamics and Infectious Diseases. Today she and I precepted the 3rd year pharmacy students at Mulago and it was really nice to hear her thoughts about antimicrobial use and find out they are in line with mine. If you want to learn more about that, check out my Blog from a couple of days ago.

4th Year students consult with each other while they review a patient’s medical record at Mulago Hospital
Finally, this afternoon I spent several hours at the Pharmaceutical Society of Uganda (PSU) in a meeting to design a pilot project to implement Pharmaceutical Care in a few hospitals. It was a really interesting meeting but as we talked through all the steps, we realized the project is larger than we first imagined. Since my talk for the Intern Supervisors here a couple of weeks ago and my talk and Cathy’s at the PSU Annual General Meeting last week, the momentum to implement Pharmaceutical Care in hospitals has grown, which prompted the meeting today. Although, there are some significant challenges to overcome.

4th Year students at the bedside of a patient at Mulago Hospital as they interview the patient to learn about the medications the patient was on at home.
The literature is filled with reports of how pharmacists can positively impact patient care and the economic use of drugs, but we need to plan a study that will show this is also possible in Uganda. To demonstrate this we will need access to data that may not be reliably collected. For example, when pharmacists are involved in direct patient care as a member of the healthcare team, safe medication use is improved. One way to measure this would be to see if the reports of adverse effects from drugs that have either been used inappropriately or given in the wrong dosage because the patient had impaired kidney function decreases after the onset of the Pharmaceutical Care project. In the USA, these reports are routinely documented and it is actually required by our accreditation bodies that we report this data.

4th Year students at the bedside of a patient at Mulago Hospital as they interview the patient to learn about the medications the patient was on at home.
In Uganda, no one requires such reporting and even if they did, there probably wouldn’t be a way to enforce this. This is a regular problem with many issues they face. There may be great policies put in place about the way drugs are dispensed or prescribed but there is no infrastructure able to enforce such regulations. An example is the dispensing of Antibiotics without prescriptions by the pharmacies as I mentioned in my last blog. The Pharmacy Act provides a list of drugs that must not be dispensed by pharmacies without a prescription, but there is no way to enforce this policy hence antibiotics are routinely sold without prescription and no evidence of a bacterial illness in a patient. Another issue that Pharmacists can really help with is finding out exactly what medications the patient was on prior to admission to the hospital to make sure the appropriate drugs are continued and the ones no longer needed are stopped. This is called “medication reconciliation” and is one of the key practices I’m teaching the students. While rounding with them this week, they were able to determine that the HIV medications the patient was on at home were different than those written for in the hospital. The physician team had somehow made a wrong assumption about his therapy and if we had not intervened, the patient would have received the wrong HIV medications. Though there are many challenges to the systematic implementation of Pharmaceutical Care, I think that the group that met today will do their best to address the barriers and will come up with a solid plan to both measure baseline data regarding the safe and rationale use of medications and then a pilot study design that will show the benefits of pharmacists being more involved with patient care.
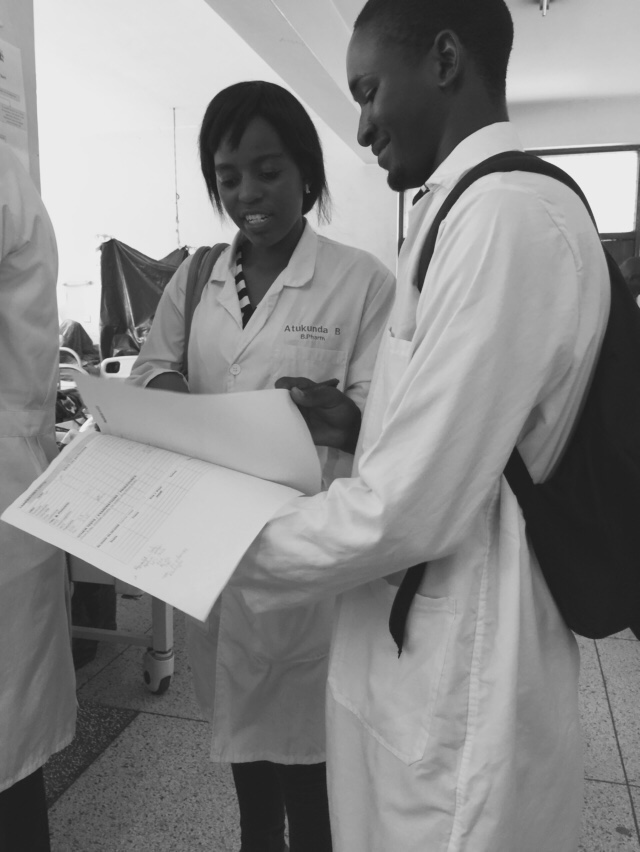
4th Year students consult with each other while they review their notes from a patient interview at Mulago Hospital
